advertisement


Editors Selection IGR 12-3
Response


Comment by Rotchfold & Anthony King on:
68907 Validity of the Monocular Trial of Intraocular Pressure-Lowering at Different Time Points in Patients Starting Topical Glaucoma Medication, King AJ; Rotchford AP, JAMA ophthalmology, 2016; 134: 742-747
See also comment(s) by Kaweh Mansouri • Luciano Quaranta • Tony Realini •We would like to thank Professor Weinreb and the IGR editorial board for selecting our work for discussion. We very much appreciate the reviewers' comments and observations about our paper.
The monocular therapeutic trial (MTT) was introduced to provide a simple, pragmatic and clinically useful method of evaluating the effectiveness of glaucoma drops. However, as the commentators have highlighted its validity has been questioned. To address this gap in the literature we undertook this study, which was designed to address some of the issues raised regarding the validity of MTT and establish whether it was indeed a useful clinical tool.
Although, as mentioned, diurnal variation is an important aspect of IOP measurement, this work is not primarily about diurnal behavior of IOP but about day-to-day variation. It is the day-today variability (which is the cause of mean regression) that impinges on our ability to determine the effectiveness of therapy. However, this day-to-day variability becomes less important if the variability is symmetrical between the eyes - thus allowing one eye to effectively be used as a control when initiating therapy.
Dr. Mansouri's comments regarding the assumptions necessary are important and we can go one step further. There is, in fact, a single combined assumption i.e. that as long as between eye day-to-day repeatability is greater than within eye repeatability, the MTT will provide a more accurate estimate of effectiveness. This (new) table showing within and between eye variances and coefficients of repeatability derived from them illustrates this point (Table 1).
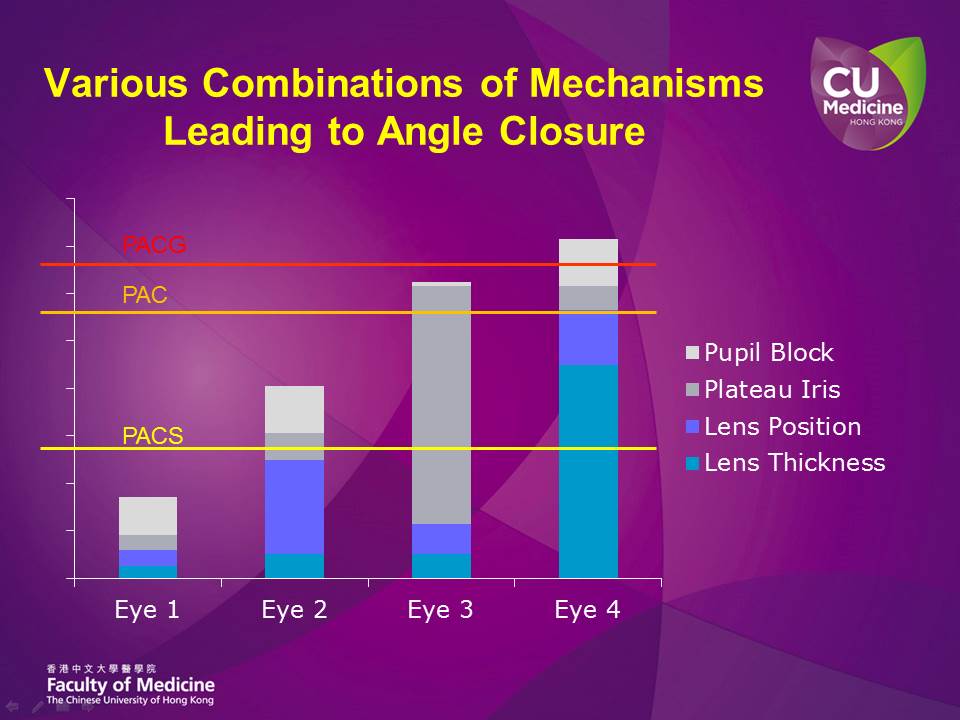 Fig 1:Various combinations of mechanisms leading to angle closure in different eyes. The height of each column reflects the extent of predisposition to angle closure in that particular eye. The eyes in this figure are hypothetical.
Fig 1:Various combinations of mechanisms leading to angle closure in different eyes. The height of each column reflects the extent of predisposition to angle closure in that particular eye. The eyes in this figure are hypothetical.
I.e., Sa2 > Sb2 indicating that repeatability between fellow eyes is greater than within eye repeatability at all time points in our study. The CR can be interpreted as meaning that, for example that at 4 pm, 95% of repeated intra eye measurements on different days would lie within a range of 8.5 mmHg whereas between 95% of fellow eye measurements lie within 4.7 mmHg of each other.
We chose to undertake our study on treatment naïve patients and to use a prostaglandin analogue to minimize the influence of other factors in our evaluation. In addition, this is important and relevant as prostaglandin analogues are normally used as the first line of therapy in treating raised IOP. We accept the limitations of the current study in patients commenced on β-blockers and limits the utility of our findings in this group of patients. We agree with Dr. Quaranta's comments regarding the variability of IOP, however, it is important to remember that the repeatability of GAT is not perfect either. In fact it is around 2 mmHg itself. This 'noise' is obviously not patient-related and represents the absolute limit of repeatability even if there was no variation in subjects' IOP at all. In this context this level of concordance is more than 'fairly high'. And it is unlikely that one would ever be able to identify absolute concordance even if it did exist because of this measurement constraint.
We compliment Dr. Realini on his robust denial of the value of the monocular trial - indeed it is perhaps that we are referring to two very separate interpretations of the monocular trial that leads us to disagree with each other. We consider that the monocular trial is a therapeutic tool used to evaluate the immediate effect of a therapeutic intervention, we do not believe that the value of the trial should be measured on its ability to predict long term IOP control or variability.
Dr. Realini suggests our findings may be attributed to a type-2 statistical error. We assume he means a type-1 error. We feel this is most unlikely, given the strength of the effect at three different time points.
We cannot claim that the MTT will predict a therapeutic effect with 100% accuracy. But it is more accurate than the usual practice of bilateral treatment initiation and comparing a single preand post-treatment pair of IOP measurements. In this patient group we previously showed that a single pair of pre- and post-treatment measurements give an estimate of treatment effect with repeatability of ± 73% (± 5.5 mmHg), which we think is not precise enough.1We would agree that it is more accurate to undertake multiple pre- and post-treatment measurements to truly establish the value of a therapeutic intervention. This is indeed what we did for comparison in our study. However, as we have also previously shown, even increasing the number to three pre- and three post-treatment measurements (i.e., six clinic visits) only increased the precision to the same level of precision achieved using the MTT (± 41%) which requires only two visits.1
One day we may have an affordable and effective means of continuous IOP monitoring to offer our patients but in the meantime, for those of us who work in healthcare contexts that cannot support the burden of so many additional appointments, the MTT, if used correctly, provides a practical and effective alternative.
References
- Rotchford AP, King AJ. Repeatability of measurements of effectiveness of glaucoma medication. Br J Ophthalmol. 2012;96(12):1494-1497.
Comments
The comment section on the IGR website is restricted to WGA#One members only. Please log-in through your WGA#One account to continue.Log-in through WGA#One
